URO-ONCOLOGY
HEMATURIA: Painless gross haematuria can be a symptom of kidney or bladder cancer. Therefore, it is usually investigated with an Ultrasound scan and CTU (CT urogram) to see the upper tract and a cystoscopy to see the bladder. Painful gross haematuria is commoner and may be caused by stones or infection. Other sources of gross haematuria include BPH, benign prostatic hyperplasia (usually > 55 years of age), glomerulonephritis (usually young) and vascular malformations. Radiocontrast is contra-indicated if there is renal failure or a strong history of allergy.
The main tumours of the urinary system are:
1) Kidney: adenocarcinoma, Wilm’s tumour (the later in children).
2) Bladder: transitional cell tumour, the commonest tumour of the urinary system.
3) Prostate: adenocarcinoma.
4) Testis: seminoma, nonseminomatous
5) Penis: squamous cell carcinoma.
KIDNEY:
Adenocarcinoma(or RCC, renal cell carcinoma, usu CCC, clear cell carcinoma)
Presentation: Gross painless haematuria; renal mass.
Investigations: CT shows a solid mass
Ultrasound to distinguish solid tumour from cyst, see IVC and renal vein invasion by tumour thrombus (feature of RCC).
CXR
CT Abdomen Thorax, esp to see para-aortic lymph nodes.
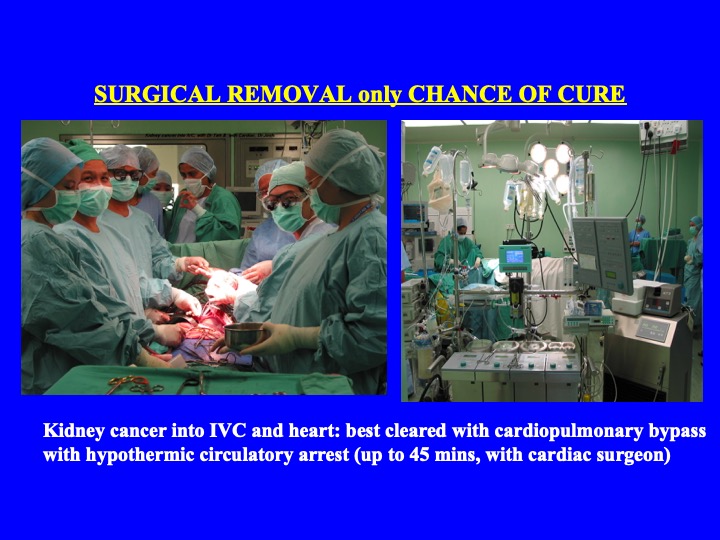
Management: Surgical removal is currently the only hope of cure. This is possible in locally confined disease; embolus present in the renal vein/IVC can be removed with the cardiac surgeon. Chemotherapy and radiotherapy are not effective. Immunotherapy (e.g. interleukin-2) and kinase inhibitors (eg sorafenib, sunitinib) is useful for metastatic disease.
PARTIAL NEPHRECTOMY is gaining popularity, especially if need to preserve nephrons to avoid dialysis.
In Wilm’s tumour, chemotherapy has important role and hence, important to manage with paediatric oncologist.
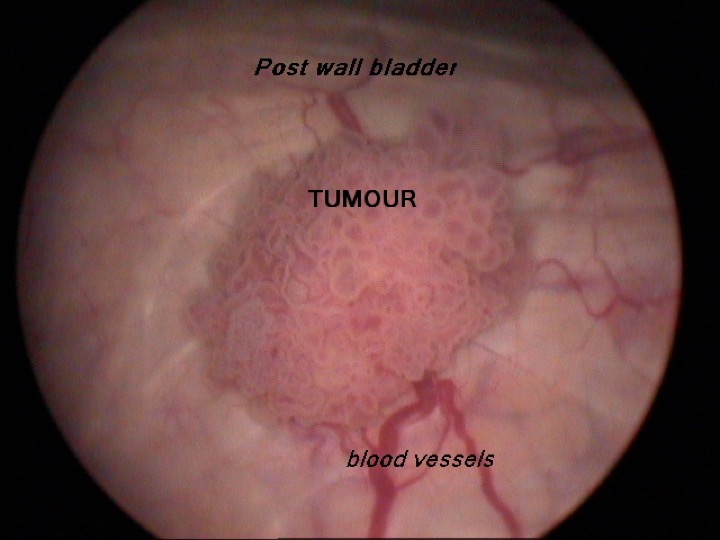
BLADDER:
Clinically commoner then cancer prostate in Malaysia. Usually TCC (transitional cell carcinoma). Almost ALL tumours in the bladder are TCCs.
Presentation: Gross painless haematuria; suprapubic mass rarely (i.e. unusual to have clinical signs).
Aetiology: Smoking increases risk 4 x
An ‘industrial disease’ where aromatic amines wereused e.g. in rubber/dye industries.
Investigations: (1) Ultrasound
(2) CTU
(2) CT TAP, thorax, abdomen and pelvis,
Management: Depends on stage and grade:
(a) NMIBT, non muscle invasive bladder tumour – transurethral resection (TURBT, transurethral resection bladder tumour). May reduce recurrence with immediate intravesical Mitomycin C /BCG; weekly x6 and maintainence
(b) Bladder Muscle Invasive – radical surgery to remove bladder and urinary diversion. Radiotherapy if not fit for surgery. 5-year survival: 50%. Grade 3 TCC especially if associated with CIS (carcinoma in situ) may be treated with radical surgery. Urinary diversion may be with ileal conduit, orthotopic neobladder or continent cutaneous stoma (eg with appendix)
(c) Advanced (locally fixed, node positive or metastatic) – palliative chemotherapy.
Note: T.C.C. may be found occasionally in other parts of the urothelium e.g. ureter and renal pelvis.
cessation of smoking important
PROSTATE:
Radical differences in mortality (e.g. very low mortality in Japanese) may be related to genetics, diet & lifestyle.
Presentation: If early, detected by blood test, PSA (prostatic specific antigen). If advanced, urinary retention, bone pain from secondaries.
Investigation: Biopsies: transrectal ultrasound guided, occa transperineal
X-ray (pelvis) osteosclerotic lesions (Ca prostate is the commonest cause of such lesions).
CT TAP
MRI
Bone Scan.
Management: (a) Localised disease: radical prostatectomy (or radiotherapy) if life expectancy > 10 years as disease may be slow growing. Robot assisted laparoscopic radical prostatectomy (RALRP) is the preferred treatment for localized disease. In low grade low volume disease with slow PSA doubling time, active surveillance may be an option.
(b) Advanced disease (local invasion, node +ve, metastatic) palliation by androgen deprivation. This may be surgical (orchidectomy) or medical (injection LHRH analogue 3 monthly). Localised bone pain can be treated with radiotherapy.
TESTIS:
Presentation: Testicular mass in young men – any SUCH MASS SHOULD BE CONSIDERED MALIGNANT UNLESS PROVEN OTHERWISE.
Aetiology: A maldescended testis has a higher incidence (5%), patients with such a history should do TSE (testicular self examination) monthly; usu. a cancer of young men.
Investigation: Ultrasound – to determine that the swelling is actually testicular (and not, e.g. a hydrocele).
Tumour markers – alpha-fetoprotein, beta-HCG (raised in teratoma), LDH.
Management: Radical orchidectomy as biopsy – inguinal route mandatory to control vascular pedicle to prevent tumour embolisation. When diagnosis confirmed, to stage tumour with CT TAP
CHEMOTHERAPYIS THE MAINSTAY OF TREATMENT AND OFTEN CURATIVE.
PENIS:
Presentation: Penile ulcer and growth, often in an advanced state although the penis is an easily visible and often used organ.
Aetiology: Circumcision in infancy gives complete immunity.
Investigation: Biopsy (including inguinal lymph nodes if these are enlarged).
Management: Surgery, chemo and radiotherapy.
Seminar on 18 February 2019
ADJUNCT PROFESSOR
UNIVERSITI MALAYSIA SARAWK
Dr Clarence Lei Chang Moh, FRCS Urol,
Consultant Urologist,