























The author joined full time urological practice in January 1987 and was also actively involved since then as an office bearer of the Malaysian Urological Association (MUA), initially as its honorary secretary. The events prior to 1987 are extracted from the archives of MUA and interviews with senior urologists.
The Malaysian Urological Association was formed on 23.7.1974 with the main office bearers as David Chelvanagam and the late G Sreenevasan. The main training centre was the Institute of Urology and Nephrology, GHKL. Since its inception, the MUA has a strong exchange programme with Australia, cumulating with an MOU signed on 22.2.2007. The urology training before 2000 was an apprenticeship type of training for 4 years, with Dato Dr Khairullah Abdullah as Head of Urology for almost two decades. The first Board of Urology of Malaysia exam was held in 2000. Since 2008, the Royal College of Physicians & Surgeons of Glasgow (the College being established in 1899) was invited to participate. This led to the conjoint award of board certification as well as a FRCS (Urol) , which is recognised by the General Medical Council of the UK. The programme had also attracted candidates from overseas including Singapore, Brunei, Myanmar and Sudan. However, the number of urologists trained is still a handful per year. In 2016, the Ministry of Health encouraged the intact of new trainees who have passed their MRCS. In tandem with this, a new curriculum & training structure is spearheaded by the current president of the MUA, Selvalingam as well as national urologist of the Ministry of Health, Rohan Malek. Most urologists resign to go to the private sector. A new flexi working hours was implemented on 1.1.2018 such that the specialists need work only 4 days in the government hospitals. The MUA also enhances the government initiative of PPP, Public Private Partnership in a working paper that was approved by the Ministry of Health on 13.11.2017.
New trainees are now taken in after the MRCS (4 to 5 years after medical school) and undergo training in a unified (public and private) urology service of Malaysia.
|
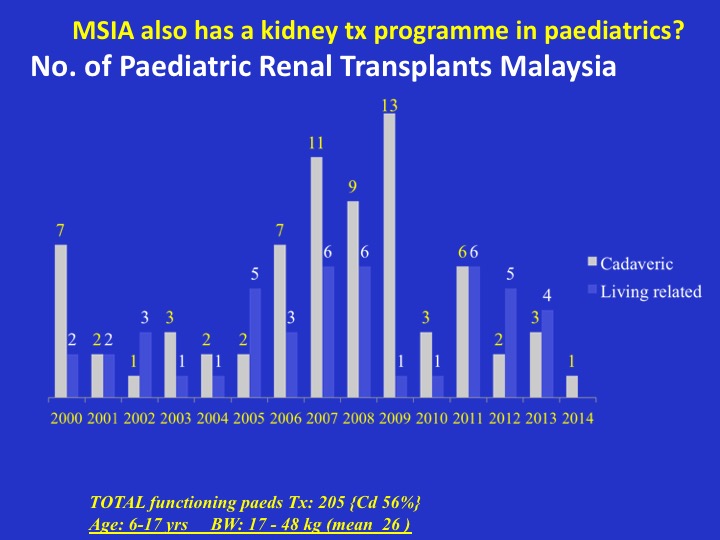
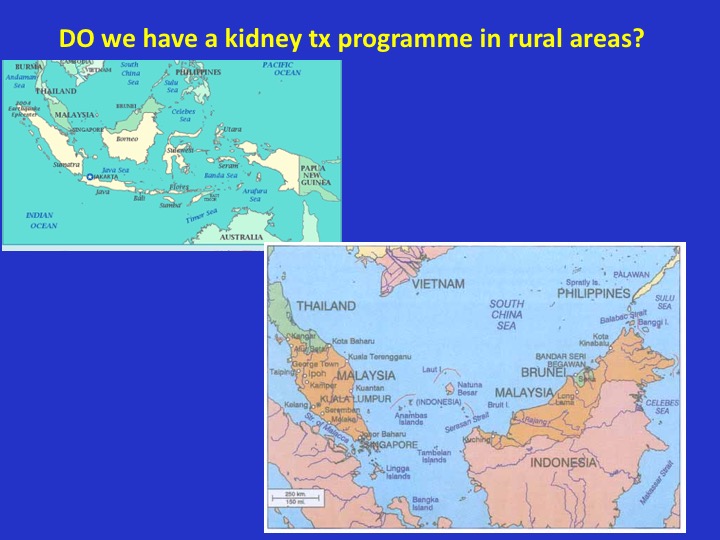
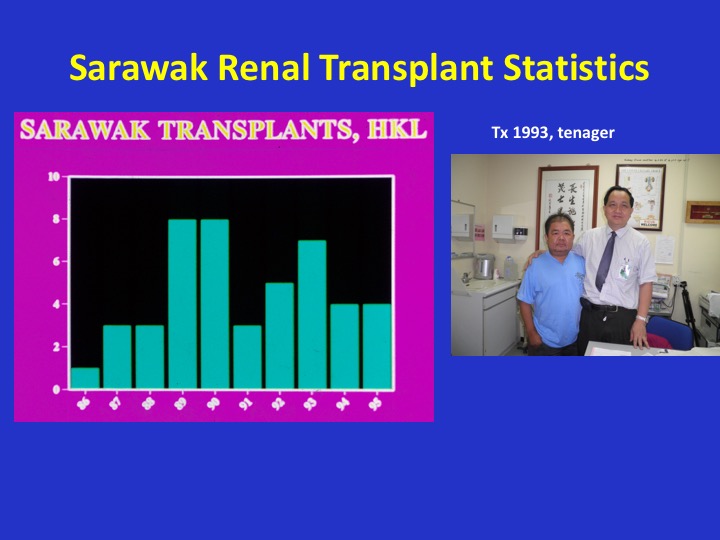
The objective of this presentation is to review & improve the current status of kidney transplantation, especially from the perceptive of the rural Sarawak. The data is from the author’s personal involvement with kidney transplantation in Malaysia since 1987, updated with data from the National Renal Registry (www.msn.org.my/nrr) & National Transplant Resource Centre (www.dermaorgan.my). Haemodialysis and peritoneal dialysis have been available since the Institute of Urology and Nephrology, GHKL was set up in 1974. Indeed, the first kidney transplant in Malaysia was done on 15.12.1975 for a teenager whose donor was his adolescent younger brother, from rural Bau of Sarawak. Since then, about 50 transplants were done yearly. There were only sporadic cadaveric transplants until cadaveric donations picked up in 1998. In the early 1990s, the average number of transplants from rural Sarawak was about 6 per annum, with a handful contributed in the later years by the cadaveric programme. In 2015, the deceased organ donors in Malaysia was still very low, 0.6 per 1 million population, whereas it is 39.7 in Spain. In neigbouring Indonesia, the kidney transplant programme only took off in 2011 when Cipto Hospital in Jakarta reported 491 transplants (mostly living related) for the period from 2011 to 2017. However, there are 11 other centres across Indonesia doing only a handful of transplants per year. Kidneys are ideally suitable for transplantation across distances as the kidney can tolerate cold ishaemia of up to 48 hours. However, a review of literature indicated that patients who are of lower educational status and living in rural areas (even in USA, JAMA. 2008;299(2):202-207) are less likely to be on the waiting list and to be transplanted. The problems confronting renal transplantation in rural areas may include: the lack of transplant medical personnel, lack of coordinating teams, lack of funds especially for the transportation of the medical team & patients in rural areas. In addition, the patient factor may include education and cultural attitudes adverse to organ donation and transplantation. As the earning power and the insurance scheme for rural areas are less, economic priorities may have to be concentrated in other areas of need, e.g. communicable diseases, cancers, accidents, maternal and child health. There is a need to intensify the multi-prone strategy which includes significant government funding as well as community involvement.
|